Last updated by The POOG on November 25, 2021.
The topic of masks is one on which not much research could be found. Without solid studies to support policy, governments end up relying on ‘experts’ and the results to date have been notoriously unreliable, with positions changing sides like a puck in a hockey game.
In order to evaluate the efficacy of masks, we need to understand what they are being used for. We will first discuss the modes of COVID-19 transmission. Then we will be able to address such questions as design and materials. Finally, we then assess their efficacy.
Modes of Disease Transmission
Surface contact is well understood as a form of transmission. The length of time the virus can persist in a viable form on various surfaces has been well studied. The resulting commendation is to wash your hands frequently in a prescribed manner and use hand sanitizers.
The other form of transmission is airborne and this is broken down into two categories, droplets and bio-aerosols. An extensive industry study[10] of the the two by Production Automation Corporation (PAC) gives the reader background on the two classes of airborne transmission. In particular, it reviews the literature on bio-aerosols. As well, consider an article by Mackay (2020)[11] and Debczak (2020)[14].
A study[13] by the CNFU reviewed 4 dozen articlesa and papers.
A NASEM Rapid Expert Consultation[5] discusses both forms of airborne transmission in the context of cloth masks worn to protect the public from the wearer.
Droplet Transmission
When you cough or sneeze, the force of the action can cause one to expel droplets of water or mucous. On one end of the spectrum, they are large enough to be visible and felt. On the other end, they may not be visible but can still be filtered out by some materials.
The droplet’s size has two important considerations. Each droplet is large enough to carry a heavy viral load. On the other hand, due to their size (and weight), they do not travel far due to gravity. The two metre rule is a heuristic for protection from coughing and sneezing.
Aerosol Transmission
Aerosols are formed by normal exhalation of fine droplets not visible to the naked eye. If you breath closely on a window, it will fog up due to the fine fine droplets of moisture that you normally exhale. In an infected person, these very small droplets can carry virus particles.
As mentioned above, the PAC paper[10] reviews several studies that support aerosol transmission of COVID-19.
Justin Morgenstern did a large survey of the literature on aerosols and disease transmission.
Due to the particle size, they remain in the air longer, especially if there are air currents that they are floating on. The implication of this is that they travel considerably farther than the larger droplets. Because they remain airborne longer, they can build up a concentration in closed spaces such as buses, trains and subways. Prolonged exposure in such an environment can give one a heavy viral load.
The nature and behaviour of aerosols is dependent on many factors related to the virus, human physiologic, droplet size, and the environment, making studies and remedial strategies complex.
At the political level, policy based on an aerosol transmission mechanism continues to be mired in confusion with bodies like the CDC flip-flopping several times in their assessment[19].
Disease Transmission and Children
It has been known from early tabulation of epidemiological data that children as an age cohort, suffer the smallest number of deaths. Of the reported deaths, we do not know if death was due to a preexisting comorbidity or not. That data may not exist, but were it to be factored in, deaths due to COVID-19 alone for children in some populations might be zero.
In any case, I have been reading reports over the last few months that children have a low rate of infection and a low rate of transmission compared to the population at large. I’m starting to collect these[30].
Asymptomatic Transmission
Not a lot is known about asymptomatic transmission. However, in Wuhan China, a city-wide SARS-CoV-2 nucleic acid screening program, from May 14 to June 1, 2020, tested 9,899,828 (92.9%) of residents, aged six years or older. 9,899,828 (92.9%) participating. From this program, Cao et al (2020) reported:
No new symptomatic cases and 300 asymptomatic cases (detection rate 0.303/10,000, 95% CI 0.270–0.339/10,000) were identified. There were no positive tests amongst 1,174 close contacts of asymptomatic cases. 107 of 34,424 previously recovered COVID-19 patients tested positive again (re-positive rate 0.31%, 95% CI 0.423–0.574%).
Cao, et al, (2020)
We added emphasis to the remarkable results which indicate no asymptomatic transmission.
Johansson et al (2021)[36] used a 30% of the population as asymptototic with a 75% rate of infection giving an over all rate of infectiveness as 23%.
The baseline assumptions for the model were that peak infectiousness occurred at the median of symptom onset [5 days] and that 30% of individuals with infection never develop symptoms and are 75% as infectious as those who do develop symptoms.
Johansson et al (2021)[36]
Types of Masks
Disposable medical masks (surgical masks) are loose-fitting devices that were designed to be worn by medical personnel to protect accidental contamination of patient wounds, and to protect the wearer against splashes or sprays of bodily fluids.
Respirators such as N-95 and P2 masks are tight-fitting masks that can protect the wearer from fine particles, providing better protection against virus exposures when properly worn. An article by Eric Litke[12], explains about N-95 mask effective filtration:
N95 masks actually have that name because they are 95% efficient at stopping particles in their least efficient particle size range — in this case those around 0.3 microns.
Litke (2020)
They are actually more effective at stopping particles smaller than 0.3 microns.
A third type of mask is the reusable cloth mask used in the community, rather than disposable medical masks, because of cost and availability. Studies of their efficacy were hard to find and only in comparison with other mask types. We did find a filtration study[16] that showed a wide range of aerosol filtering ability based on design and materials. It should be noted that this only indicates filtering efficiency and not aerosol protection which is also highly dependent on fit and mask maintenance.
Roger Koop, in a long dissertation[24], makes a number of good points on masks:
- NOT designed to filter infectious agents but rather inert particulates
- Designed for normal breathing patterns, not exertive force.
- Designed for minimal usage time. They are NOT intended to be stuck on your face for hours.
- People who have experienced this virus do NOT need to wear face coverings.
- Children should not be wearing face coverings.
- In the open environment, no one should be wearing face coverings.
- The “Mask Mandate” idea is a truly ridiculous, knee-jerk reaction and needs to be withdrawn and thrown in the waste bin of disastrous policy, along with lockdowns and school closures.
- There may be other health risks associated with continued use of face coverings.
Discussion of Results of Studies Cited
Xiao et al. (2020) reviewed the evidence from 14 randomized controlled trials of standard non-pharmaceutical personal protective measures and environmental hygiene measures in non-healthcare settings. This included hand washing and the use of masks. Their results are:
We did not find evidence that surgical-type face masks are effective in reducing laboratory-confirmed influenza transmission, either when worn by infected persons (source control) or by persons in the general community to reduce their susceptibility.
Xiao et al. (2020)[1]
MacIntyre et al. (2015) compared cloth masks to medical masks. cloth masks and found that:
Penetration of cloth masks by particles was almost 97% and medical masks 44%.
Cloth masks resulted in significantly higher rates of infection than medical masks, and also performed worse than the control arm [of the study].
MacIntyre et al. (2015)[2]
Another study by MacIntyre et al. (2011)[3] compared the efficiency of N-95 masks, both fit-tested and non-fit-tested to surgical masks. They found no significant difference between the two N-95 groups which suggests that arguments against the use of N-95 masks by the public due to fitting issues are bogus. They found that:
infection were consistently lower for the N95 group compared to medical masks. … There was no significant difference in outcomes between the N95 arms with and without fit testing.
MacIntyre et al. (2011)[3]
Brosseau, and Sietsema (2020)[4] (also MacIntyre et al. (2015)[8]), surveyed the publish literature on cloth masks, noted its scarcity, but stated:
We do, however, have data from laboratory studies that indicate cloth masks or face coverings offer very low filter collection efficiency for the smaller inhalable particles we believe are largely responsible for transmission
Brosseau, and Sietsema (2020)[4]
Quesnel (1975) tested 5 types of surgical masks and found that:
the gross efficiency of all the masks was high, but that some masks were distinctly better at small particle “filtration” than others.
Quesnel (1975)
Yang et al. (2011)[6], in a study of health care workers in small and large hospitals found “the protective efficacy of medical masks is better than that of cotton yarn ones“.
Chughtai et al. (2020) found that “cloth masks may provide some protection if well designed and used correctly“. Their statement “In community settings, however, cloth masks may be used to prevent community spread of infections by sick or asymptomatically infected persons” is a false conclusion since they demonstrated no ‘preventative’ benefit.
The most extensive and readable review of research on mask use is one put together for Councillor Michael van Holst of London, Ontario, Canada[25]. Keeping in mind that the studies cited above place cloth masks well behind surgical masks in terms of efficacy, and that most of the research in this report is on surgical masks, the cnclusion he quotes from a studty by Klompas et al sums up the whole picture:
“wearing a mask outside health care facilities offers little, if any, protection from infection.”
A Danish study[28] showed marginal effectiveness in protecting a wearer of a surgical mask if other protective measures are in place. However, statistically, the results were “not significant“. There conclusion was:
… a recommendation to wear a surgical mask when outside the home among others did not reduce, at conventional levels of statistical significance, incident SARS-CoV-2 infection compared with no mask recommendation.
Bundgaard et al (2020)[28].
Fisher et al. performed a study of of 154 hospital outpatients who had been infected with SARS-CoV-2. 108 or 70.6% had always worn a mask in the 14-days prior to the onset of symptoms. In contrast, only 6 or 3.9% of those treated had never worn a mask during the 14-day period. This is a remarkable result that raises serious questions about the wearing of masks and invites further research.
There are articles of a meta-study nature that conclude masks have little no no value in stopping the disease[29].
A Danish study[38] by H Bundgaard and JS Bundgaard in an environment where personal mask use was uncommon observed that (emphasis added):
In this community-based, randomized controlled trial conducted in a setting where mask wearing was uncommon and was not among other recommended public health measures related to COVID-19, a recommendation to wear a surgical mask when outside the home among others did not reduce, at conventional levels of statistical significance, incident SARS-CoV-2 infection compared with no mask recommendation.
Bundgaard and JS Bundgaard (2021)[38]
They also noted that “the trial did not test the role of masks in source control” and no conclusion on value of such can be made.
Source Control As Virtue Signalling and Shaming
We’ve gone through cycles where the same authorities have told us that “masks don’t work”, then “masks work”. Very recently the narrative around masks has bifurcated to “masks don’t protect you from others” but “masks protect others from you”. Or in other words, “I must wear a mask so that I can’t give you what I don’t have”.
Apart from sounding like a strategy invented in the boardroom of a Wall Street advertising firm, it doesn’t hold up to scrutiny.
The National Academies of Sciences, Engineering, and Medicine (NASEM) was recently instructed to do a Rapid Expert Consultation with the objective:
The aim of this rapid expert consultation is to respond to your request concerning the effectiveness of homemade fabric masks worn by the general public to protect others, as distinct from protecting the wearer.
… in terms of their ability to reduce viral spread during the asymptomatic or presymptomatic period.
Besser et al. (2020)[5]
Someone was in a hurry to find ‘scientific’ evidence to support the new narrative. The authors note that:
in addition to being spread by respiratory droplets that one can see and feel, SARS-CoV-2 can also be spread by invisible droplets, as small as 5 microns (or micrometers), and by even smaller bioaerosol particles.
ibid.
The NASEM finding from a review of studies in the literature, concluded that the “current level of benefit, if any, is not possible to assess.” The studies generally tested filtration properties of various materials.
Of specific studies and findings, one noted that “both homemade and surgical masks reduced the number of large-sized microorganisms expelled” while another noted that “N95 masks provided 25 times the protection of surgical masks and 50 times the protection of cloth masks.”
For a general discussion on the topic of the validity of studies, read the Anderson article[41]. He reviews a number of studies. The summary conclusion would be that masks show no statistically significant benefit.
Negative Impact of Mask Use
There are a few reports hypothesizing negative health risks from using masks as well as environmental impacts[26][27]. The most common one is the buildup of bacteria or virus pathogens on or in the mask that may then be re-transmitted by touching or breathing[17].
The following 5:49 minute video is by a doctor discussing the negative impacts of wearing a mask.
Another common concern expressed is the decrease in blood oxygenation leading to impaired physical and mental functioning and permanent neurological damage[23].
Further, there can be a buildup of deadly pathogens on masks[40].
The Political Dimension of Masks
There is a body of opinion that posits that forced wearing of masks is part of a larger plan of psychological fear and control of the population[18]. We explore this idea further in topics under our PsyOps category[20].
Summary
Studies on the use of masks and respirators in clinical and community settings are few, particularly given the number of variables such as materials, fit, and diseases to be protected from. There are some laboratory studies of filtration by different materials and mask types.
In general, N-95 masks offer better protection over medical or surgical masks (25 times) and cloth masks (50 times). Fit testing of N-95 masks offers no additional advantage, nullifying the argument against their use by the general public that the latter can’t fit them properly if simple directions are followed.
Medical masks offer a degree of protection for droplet and fluid transmission but little protection from aerosols. A 1975 study of 5 types which showed a wide range of effectiveness has hopefully informed an optimal standard for production. These conclusions are born out by the extensive CFNU study[13]. WHO guidance[31], p.8, cites two major studies that found either no benefit to mask wearing or little to no benefit. They did cite smaller studies and reports that indicated partial protection to wearers in high risk situations.
Cloth masks, based on the limited testing available, have shown to be largely ineffective, particularly given the lack of manufacturing standards. As the NASEM report notes, overall, cloth masks offer some reduction in the number of large-sized particles expelled but little efficacy for stopping aerosols.
There are, however, some advocates of universal masking over the use of social distancing, for both source control and general protection[15].
Finally, NASEM states that the current level of benefit [of cloth masks], if any, is not possible to assess. This means that there is no scientific basis for the current virtue signalling policy of cloth mask use. Overall, they are only marginally effective in preventing disease spread.
The Epidemiological Evidence: Mask Mandates Don’t Work
Jordan Schachtel writing in The Dossier[33], cites data that shows in 8 of the largest US metropolitan areas, mask usage in the population is 94% or higher while cases are rising. Other data shows that mask mandates have no discernible effect on case numbers:







Here are additional mask charts from the rational Ground. Also see their Interactive Tool: Masks & COVID-19. Others have observed the apparent lack of correlation between mask wearing and disease transmission[34].
Fögen[35], in a paper not yet peer reviewed, found that mask mandates increase case fatality rates over non-mandated counties by a factor of 11 times.
… mask mandates in Kansas counties during the summer of2020 actually increased case fatality rate significantly compared to Kansas counties without mask mandates.
… the case fatality rate by SARS-CoV-2 is as low as 0.026% in Kansas counties without mask mandates, but 0.286% in Kansas counties with mask mandates, resulting in a highly significant risk ratio of over 11.
Fögen[35]
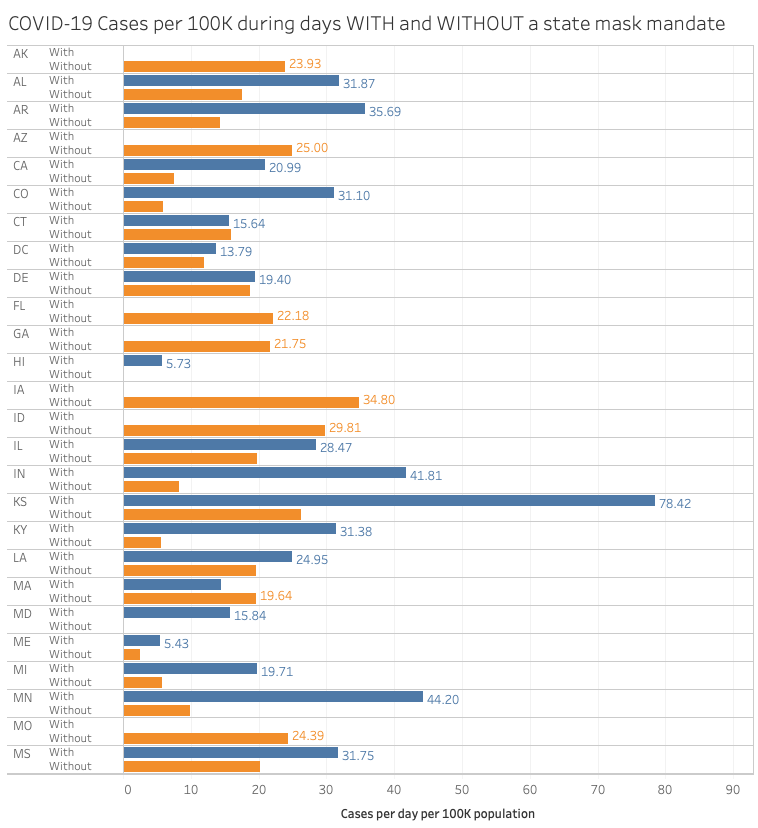
Justin Hart provides the following data that shows that states in the US that hav had periods with and without mask mandates had more caases after the mask mandate was enacted.
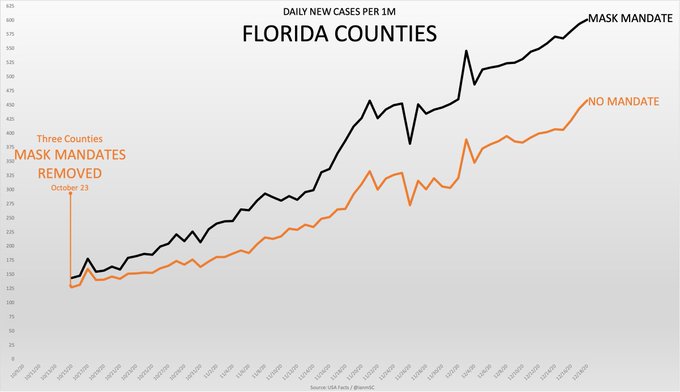
Another graph off of twitter by the person ‘IM’ shows a similar pattern for three Florida counties:
Other researchers have arrived at similar conclusions[37][43].
Mask Usage and Other NPIs
When considering the full set or at least a major subset of NPIs, we are faced with a multivariate problem difficult to analyze. Comparison of different jurisdictions with different NPI usage is the most common approach. A lack of correlation between infection cases and various NPIs, particularly more restrictive ones like lockdowns with and without mask usage has been noted[39].
Comment
The rational approach to disease management is fourfold.
- Act quickly to put in place actionable measures to protect the elderly and those at high risk due to comorbidities.
- Ensure proper and adequate protection measures are available to the public including vaccines, pharmaceuticals, and neutraceuticals such as Vitamin D3.
- Educate the public on the risk that they face both in contracting the disease and in infection outcome. Stop propagandizing the public. Enough research has been done on masks to make an informed recommendation on mask usage.
- Allow each individual to make their own risk assessment and response. Lockdowns may only at most be justified as an initial emergency response until the other measures can be developed and implemented.
Addendum
I did most of my research on masks over a year ago and have no reason to expect that the general results will change. These are that, given that aerosol transmission seems to be the acccepted mode with droplet transmission a theoretical means but not the predominant means, cloth masks are ineffective and surgical masks may be marginally effective depending on the study cited.
Therefore, new research, unless ground breaking will simply be noted here through the references[41][42].
References
to educate the public on the risk that they face both in contracting the disease and in infection outcome. Enough research has been done on masks to make an informed recommendation on mask usage.
- Xiao, J., Shiu, E., Gao, H., et al. (2020). Nonpharmaceutical Measures for Pandemic Influenza in Nonhealthcare Settings—Personal Protective and Environmental Measures. Emerging Infectious Diseases, 26(5), 967-975. https://dx.doi.org/10.3201/eid2605.190994.
- MacIntyre, C.R., Seale, H., Dung, T.C., et al. (2015). A cluster randomised trial of cloth masks compared with medical masks in healthcare workers. BMJ Open. 2015; 5(4): e006577. Published online 2015 Apr 22. doi: 10.1136/bmjopen-2014-006577.
- MacIntyre, C.R., Wang, Q., Cauchemez, S., et al. (2011). A cluster randomized clinical trial comparing fit‐tested and non‐fit‐tested N95 respirators to medical masks to prevent respiratory virus infection in health care workers. Influenza. 2011 May; 5(3): 170–179. Published online 2011 Jan 27. doi: 10.1111/j.1750-2659.2011.00198.x
- Lisa M Brosseau, and Margaret Sietsema, (2020). COMMENTARY: Masks-for-all for COVID-19 not based on sound data. CIDRAP. Apr 01, 2020.
- Besser, R., Fischhoff, B., Jayaraman, S., and Osterholm, M. (2020) Rapid Expert Consultation on the Effectiveness of Fabric Masks for the COVID-19 Pandemic. National Academies of Sciences, Engineering, and Medicine (NASEM), April 8, 2020, Washington, DC: https://doi.org/10.17226/25776; PDF.
- Peng Yang , Holly Seale, C Raina MacIntyre, et al. (2011). Mask-wearing and respiratory infection in healthcare workers in Beijing, China. Braz J Infect Dis. Mar-Apr 2011;15(2):102-8. doi: 10.1016/S1413-8670(11)70153-2.
- Quesnel, L.B. (1975). The efficiency of surgical masks of varying design and composition. Br J Surg. 1975 Dec;62(12):936-40. doi: 10.1002/bjs.1800621203.
- MacIntyre, C.R. and Chughtai, A.A., (2015). Facemasks for the prevention of infection in healthcare and community settings. BMJ. 2015 Apr 9;350:h694. doi: 10.1136/bmj.h694.
- Morgenstern, J. Aerosols, Droplets, and Airborne Spread: Everything you could possibly want to know. Published -Updated .
- Droplets vs Airborne – Science of Airborne Droplets, Aerosols, Particles, and Face Masks. Production Automation Corporation, July 2020.
- Like, E. Fact check: No, N95 filters are not too large to stop COVID-19 particles. USA TODAY, June 11, 2020.
- CFNU research summary on COVID-19. Canadian Federation of Nurses Unions, updated August 4, 2020.
- Debczak, M. Airborne vs. Aerosol vs. Droplet: What’s the Difference? MF, April 14, 2020.
- Susanna Esposito, Nicola Principi, Chi Chi Leung. Universal use of face masks for success against COVID-19: evidence and implications for prevention policies. European Respiratory Journal 2020 55: 2001260; DOI: 10.1183/13993003.01260-2020.
- Abhiteja Konda, Abhinav Prakash, Gregory A Moss, et al. Aerosol Filtration Efficiency of Common Fabrics Used in Respiratory Cloth Masks. ACS Nano. 2020 May 26;14(5):6339-6347. doi: 10.1021/acsnano.0c03252.
- Russell Blaylock. Blaylock: Face Masks Pose Serious Risks To The Healthy. Technocracy News and Trends, May 11, 2020.
- Bill Willers. The Mask as a Symbol of Subjugation. Dissident Voice, July 3rd, 2020.
- Tyler Durden. CDC Re-Releases Guidance Claiming COVID-19 ‘Airborne’ Transmission Is Possible, But Less Common. ZeroHedge, Mon, 10/05/2020.
- Bill Willers. The Program to Mask Society is a Grotesque Governmental Manipulation of a Frightened and Confused Public. Global Research, 23 September 2020.
- Chughtai, A. A., Seale, H., & Macintyre, C. (2020). Effectiveness of Cloth Masks for Protection Against Severe Acute Respiratory Syndrome Coronavirus 2. Emerging Infectious Diseases, 26(10), 1-5. https://dx.doi.org/10.3201/eid2610.200948.
- Fisher KA, Tenforde MW, Feldstein LR, et al. Community and Close Contact Exposures Associated with COVID-19 Among Symptomatic Adults ≥18 Years in 11 Outpatient Health Care Facilities — United States, July 2020. MMWR Morb Mortal Wkly Rep 2020;69:1258–1264. DOI: http://dx.doi.org/10.15585/mmwr.mm6936a5.
- Henna Maria. German Neurologist Warns Against Wearing Facemasks: ‘Oxygen Deprivation Causes Permanent Neurological Damage’. SOTT Focus, Tue, 06 Oct 2020.
- Roger W. Koops. The Year of Disguise. AIER, October 16, 2020.
- COVID Research on Masks. Councillor Michael van Holst, 2020.
- Cory Morningstar. Face Masks: A Danger to Our Planet, Our Children & Ourselves. Off Guardian, November 6, 2020.
- Cory Morningstar. Willful Blindness, Hypocrisy & Planetary Repercussions. The Art of Annihilation,October 18, 2020.
- H Bundgaard, J S Bundgaard, D E T Raaschou-Pedersen, et al. Effectiveness of Adding a Mask Recommendation to Other Public Health Measures to Prevent SARS-CoV-2 Infection in Danish Mask Wearers. AIM, 18 November 2020, https://doi.org/10.7326/M20-6817.
- Are Face Masks Effective? The Evidence. Swiss Policy Research, updated: November 18, 2020.
- Stacey Lennox. Dr. Fauci Finally Confirms That Children Don’t Catch or Transmit COVID-19 in Large Numbers. PJ Media, November 29, 2020.
- Mask use in the context of COVID-19: Interim guidance. WHO, December 01. 2020.
- Cao, S., Gan, Y., Wang, C. et al. Post-lockdown SARS-CoV-2 nucleic acid screening in nearly ten million residents of Wuhan, China. Nat Commun 11, 5917 (2020). https://doi.org/10.1038/s41467-020-19802-w.
- Jordan Schachtel. Everyone Is Already Wearing a Mask. They Just Don’t Work. The Dossier, December 07, 2020.
- Editors. But, But, Masks!??…. ZeroHedge. December 20, 2020.
- Fögen F. Facemasks and SARS-CoV-2 case fatality rate. preprint retrieved December 21, 2020.
- Johansson MA, Quandelacy TM, Kada S, et al. SARS-CoV-2 Transmission From People Without COVID-19 Symptoms. JAMA Netw Open. January 7, 2021; 4(1):e2035057. doi:10.1001/jamanetworkopen.2020.35057.
- Magness PW. The Empirical Case for a Mask Mandate Lacks Scientific Grounding. AIER. January 19, 2021.
- Bundgaard H and Bundgaard JS. Effectiveness of Adding a Mask Recommendation to Other Public Health Measures to Prevent SARS-CoV-2 Infection in Danish Mask Wearers. Ann Intern Med. March 2021. https://doi.org/10.7326/M20-6817.
- Rozmajzl A. Why Is There No Correlation Between Masks, Lockdowns, and Covid Suppression? Mises Wire. May 04, 2021.
- Lab Study Reveals Deadly Pathogens Found On Children’s Face Masks
- Anderson JH. Do Masks Work? CJ. August 11, 2021.
- Steiber Z. Little Evidence Supports the Use of Cloth Masks to Limit Spread of Coronavirus: Analysis. November 15, 2021.
- Watson PJ. Oxford Professor: Official Data Shows Face Masks “Made No Meaningful Difference” to Infection Rates. Summit News. November 30, 2021.